We all understand what it feels like to have that instinctual feeling that something just isn’t right, it just feels a little bit ‘off’.
We can’t always explain why, but we have that overwhelming desire to go and ‘fix it’ in some way. We do this until we feel as though things are as they should be.
Everyone experiences this, but for someone with Just Right OCD that feeling is relentless and hard to shake.
Unlike most other OCD subtypes, Just Right OCD is driven by a sense of incompleteness or incorrectness.
Most OCD subtypes cause the sufferer to fixate on future-focused fears and outcomes. However, those with Real-event OCD – also known as ‘real-life’ OCD – is distinguished by obsessions and compulsions surrounding an event that has happened in the past.
In the case of real-event OCD, the sufferer finds themselves scrutinizing and ruminating over past events. Doubting the things they’ve said and done, leaving them with immense feelings of guilt and shame that they attempt to navigate through compulsive behaviors.
Someone with real-event OCD will exert a great deal of energy to try and find certainty around a past event which makes it very difficult to live and embrace the present moment.
Real-event OCD can feel as though it steals from the present moment as the sufferer remains in a rumination loop, trying to analyze and scrutinize past events that often leave them feeling like they are a bad person.
Here we will explore the ins and outs of real-event OCD.
But first, a quick recap of the OCD basics…
An Overview of OCD
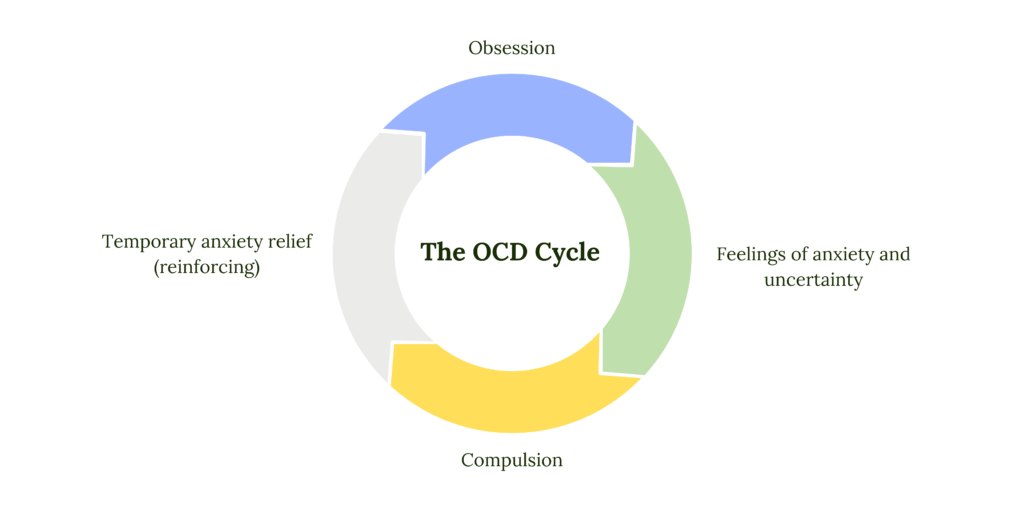
There are two core components that characterize OCD and all of the OCD subtypes.
These are obsessions and compulsions.
OCD is a common mental health condition whereby the sufferer experiences obsessions in the form of thoughts, images, urges, feelings, or sensations, which trigger extreme levels of uncertainty and anxiety.
As OCD is egodystonic – meaning it goes against our values and morals – those obsessions are disturbing in nature and leave the sufferer questioning their sense of self.
Because the very nature of these thoughts has us challenging who we are, they are perceived as a cause for concern and we believe they require our attention.
In a bid to manage the uncertainty and anxiety following these obsessions, the sufferer engages in compulsive behaviors that offer temporary relief.
Click here to join our newsletter and receive instant access to our 6-part mental compulsions series, teaching you how to resist the urge to do mental compulsions (with PDF worksheets)
These compulsions offer short-term relief but contribute to long-term struggle as they leave the sufferer trapped in the OCD cycle.
The good news is that this OCD cycle can be broken!
Effective treatment is available so you can begin managing the anxiety and uncertainty without needing to engage in compulsive behaviors.
The ins and outs of Real-Event OCD
We can all find ourselves reflecting on past events from time to time, wondering whether we should have done things a little differently.
We might berate ourselves for a moment about the things we have said or done that could have been handled more effectively.
We may even experience momentary guilt over the potential consequences of our past behaviors.
But for those without OCD, these reflections and feelings tend to fade over time. For those with real-event OCD, they find themselves over-analyzing, fixating, and ruminating on past events in a desperate plea to gain a sense of certainty.
They may be searching for definitive answers to suggest that they didn’t do anything wrong and that they aren’t a bad person.
A common compulsion within real-event OCD is mental review.
The sufferer will replay the moment over and over again.
Guilt and shame are overwhelming feelings that occur for those with real-event OCD. And these feelings brought about by such reflections are intense and painful to manage as they leave the sufferer questioning their morality and identity.
OCD takes hold of the past event and warps the sufferer’s perception, positioning them as the ‘bad guy’ or ‘villain’ of the piece, for which they can often call on self-punishment as the compulsion believing they deserve to be punished.
Examples of Real-Event OCD
Someone with real-event OCD can experience obsessions about a wide variety of past events. Anything from cheating in an exam, an argument with a partner, a job interview, or even an interaction with a stranger at the local shop.
The common thread is that obsessions are almost always driven by the fear of being a bad person.
Common Real-Event Obsessions
Did I inadvertently cause that person to feel X,Y, or Z
What would have happened if I hadn’t said or done X,Y, or Z
Was that wrong? Did I commit a crime? Am I morally corrupt?
Am I bad person for doing/saying X,Y, or Z?
It’s because I did (X) that this bad outcome occurred
I’m the reason that person I care for is suffering, because I did/said (X) when I shouldn’t have
This negative circumstance is a direct result of this thing I did/said years ago
An example of how real-event obsessions may occur could look like this…
“A friend of mine told me she kept having heart palpitations and feeling faint but I simply joked and told her she was probably just unfit. She has now been diagnosed with heart disease which they would have caught sooner if I had taken it more seriously and told her to get herself checked. If she get’s seriously ill, this will all be my fault.”
Common Real-Event Compulsions
Mental Review – repetitively playing the event over and over again in their mind to find proof that what they believe about themselves or the event is true.
Self-punishment – criticizing and berating themselves because they believe they deserve to be punished for their past behaviors.
Reassurance-seeking – Excessive reassurance-seeking from friends or family to clarify that they behaved ‘correctly’ or to confirm that they did or didn’t do anything wrong or inappropriate.
Apologizing – Someone with real-event OCD may excessively apologize to the person they believe to have wronged in the hope of gaining forgiveness.
We can use the obsession above to show an example of how the compulsion may then present.
This sufferer may replay the experience repeatedly in their mind noting what they believe they should have said or done differently. They may punish themselves by thinking, “You should have told her to see a doctor. You shouldn’t have joked about it. This is all your fault”
They may ask others whether or not they think this could have been prevented if they had told their friend to see a specialist sooner.
They may go out of their way to make up for their ‘wrong behavior’ by apologizing excessively to their friend. They may also go out of their way to do good deeds in service of the community to be forgiven for their ‘perceived error’ or ‘mistake’.
How to know if you’re experiencing Real-Event OCD?
It’s common for everyone to find themselves dwelling on past events from time to time. But here is a breakdown of symptoms to consider if you think you may have real event OCD:
Repeatedly replaying events in your mind
Over-analyzing the outcomes of your actions
Feeling excessive guilt, shame, or doubt about your actions
Apologizing excessively to those involved
Excessive reassurance-seeking to validate your experience
An intense and overwhelming feeling that you are a bad person
Someone with real event OCD can lose hours of their day ruminating and fixating on these past events.
It’s almost always impossible to gain 100% certainty, but even more so when it comes to analyzing past events that have come and gone. Because of this, those obsessions always tend to crop back up.
You can find yourself trapped in the past and unable to engage and enjoy the present moment and struggle to shake this overwhelming sense that you’re not a good person.
However, if you are able to change your relationship to those obsessions and resist the urge to do compulsions, you can find long-term relief from real-event OCD.
ERP is deemed the gold standard treatment for OCD and has been shown to be highly effective. This means that it is highly possible for you to fully recover from OCD using this treatment.
In ERP, you work with your therapist to place yourself in scenarios that gradually and intentionally trigger your obsessions. You will work together to navigate the uncertainty and anxiety and resist the urge to do compulsions.
Your brain learns that you are capable of managing anxiety and uncertainty without the use of compulsions. Each time you engage in compulsive behaviors you strengthen OCD’s hold. When you resist the urge to engage in compulsions, you can learn new ways to respond to your obsessions that will – over time – reduce the anxiety.
ERP for Real-Event OCD
Most highly trained ERP therapists will first provide thorough psychoeducation on real-event OCD and train you to engage in effective response prevention.
Response prevention is a component of ERP where we practice reducing any compulsions that the person with real-even OCD is engaging in.
Research has shown that ACT (acceptance and commitment therapy) is a highly effective modality supplement to ERP, where the person with real-event OCD practices working with value-based behaviors rather than fear-based behaviors and learns how to manage their intrusive thoughts using tools like diffusion and mindfulness skills.
In the case of real-event OCD, a common form of ERP therapy is to use an imaginal exposure script.
An imaginal script for real-event could be writing out the story as it happened, as specifically as possible, so that you can use their mindfulness, ACT, and ERP tools to resist the urge to do compulsions.
In addition, other exposures that may be helpful and beneficial are engaging back in any behaviors that you have been avoiding. You and your therapist will work together to make sure the exposures you do are exposures that you feel will be helpful and worth engaging in.
Finding a qualified therapist
Real-event OCD can sometimes be tricky to diagnose and treat. The nature of most OCD types means they are driven by the fear of what might happen in the future whereas real-event OCD is driven by the fear of what’s happened in the past.
We highly recommend you want to do your due diligence and be sure to work with an OCD specialist who is ERP trained as this is the most effective treatment for OCD and yields incredible results. It is important to work with a qualified mental health professional who can offer an accurate diagnosis and support you with the best treatment plan.
If you are based in California, our friendly team of elite OCD specialists can help you navigate your OCD and support you on your recovery journey.
Studies have shown that those with obsessive-compulsive disorder (OCD) struggle with increased rates of insomnia compared to those without OCD.
We all have sleepless nights from time to time.
The stressors of daily life can have our minds racing and us tossing and turning through the early hours of the morning. This is very common.
However, for those with OCD, obsessive thoughts can keep them stuck in a miserable cycle of not being able to switch off their minds. Trapped in a restless cycle of racing thoughts and sleepless nights, insomnia adds a new layer of difficulty when managing OCD.
Obsessive-compulsive disorder (OCD) and attention deficit hyperactivity disorder (ADHD) are two common psychiatric disorders.
A person with little knowledge of these disorders could confuse the symptoms associated with attention and concentration, believing one disorder to be the other.
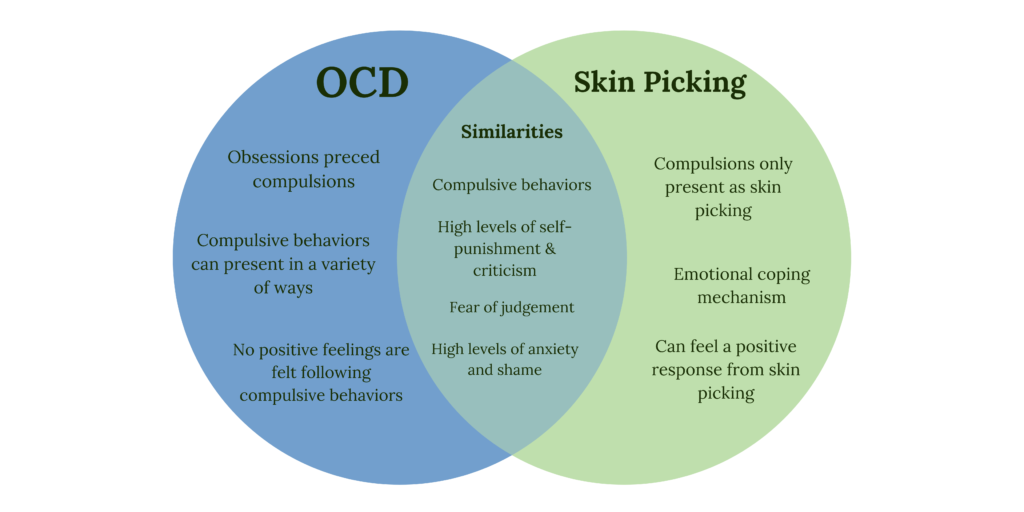
Unlike OCD which is classed as an anxiety disorder, skin-picking disorder (excoriation or dermatillomania) is known as a body-focused repetitive behavior.
Skin-picking disorder may also be known as a body-focused repetitive behavior. It may also be called an impulse control disorder due to an excessive and ongoing urge to perform the skin-picking act. And in other occasions may be named an ‘obsessive-compulsive spectrum disorder’ due to the features that overlap with OCD.
While skin-picking disorder and OCD are two separate conditions, people with skin-picking disorder are more likely to have OCD or OC spectrum disorders such as hair pulling, BDD, and tic disorders.
This is because of the urge to engage in those repetitive ritualistic behaviors that offer relief either from intrusive and unwanted thoughts, or negative feelings or emotions.
Let’s get into the differences between these two disorders…
OCD is a mental illness characterized by obsessive and unwanted thoughts or urges followed by repetitive physical or mental compulsions done to reduce the resulting anxiety.
It’s important to differentiate between everyday, low-frequency anxiety that many people will experience and disordered anxiety, brought on by these intrusive thoughts.
An intrusive thought may look something like this:
When these thoughts arise, someone with OCD feels compelled to solve for the uncertainty and anxiety that arises. This is why OCD is sometimes known as the ‘doubting disorder’.
OCD is egodystonic in nature which means the obsessions experienced by the sufferer goes against their values.
Unsurprisingly, when a disturbing thought arises, the uncertainty surrounding it can feel unbearable.
The OCD sufferer may find themselves ruminating on what this thought must mean about them and try to ‘figure it out’.
Why did I have this thought?
What does it mean about me?
What might happen if I don’t do something about it?
In an attempt to alleviate the uncertainty and anxiety brought about by this unwanted thought, the sufferer performs compulsions that offer short-term relief.
For example, someone with postpartum OCD may fear that their newborn child will stop breathing in their sleep. The compulsion might be to check on their baby at regular intervals which in turn disrupts their own sleep and has a greater knock-on effect to their mental and physical health.
Another example may be someone with contamination OCD. They may fear intrusive thoughts such as, “What if I catch a disease?” or “What if I get sick and die?”.
The compulsion in this example might be to excessively wash their hands and wipe down objects before touching them.
The disordered anxiety suffered by those with OCD can consume all aspects of their life.
Social gatherings may be avoided, relationships become strained, and work or school can become difficult to focus on. OCD can be very scary, especially if obsessions are violent in nature, but it is treatable and manageable with the right help.
Click here to sign up for our weekly newsletter and receive immediate access to the 6-part mental compulsions audio series to help you resist the urge to engage in mental rituals (PDF worksheets included)
Skin picking disorder or excoriation is characterized by the habitual picking of skin, commonly around your nails, pimples, or blemishes.
People with dermatillomania may also create open sores by compulsively touching or picking at the skin, even if there is nothing there to pick at.
We’re all guilty of occasionally picking at our skin, but it becomes a disordered condition when it is near-constant and causes bleeding, open sores, or scars.
Although, to the untrained eye, skin picking may not seem overly distressing or a source for concern, those with excoriation disorder often find themselves trapped in a difficult cycle to break.
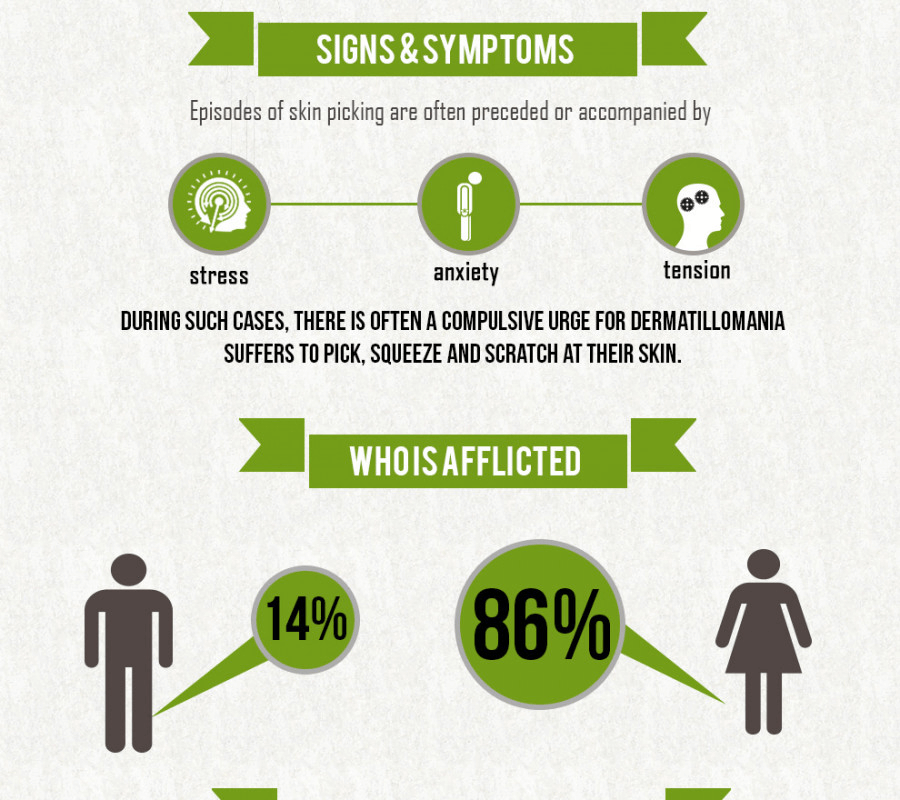
People may pick at their skin for a variety of reasons including boredom, anxiety, increased stress, or to cope with negative emotions.
While skin picking offers an initial burst of relief, it often follows with intense feelings of guilt or shame. Someone with excoriation disorder could spend hours each day picking their skin, thinking about picking their skin or trying to resist the urge to pick their skin.
It could be very easy for an observer to label this as an insignificant ‘bad habit’ but for the sufferer, skin picking can lead to greater implications that impact their quality of life.
It is not uncommon for those with excoriation disorder to avoid social events, isolate themselves from loved ones, have difficulty managing their condition at work, and fall into episodes of depression due to feeling ‘out of control’.
Are skin picking and OCD the same?
There are similarities between the symptoms of skin picking and OCD but they are not the same.
They are, however, both categorized as obsessive-compulsive and related disorders under the DSM-V (Diagnostic Statistical Manual) due to their overlapping features and the frequency with which they are simultaneously diagnosed within individuals.
It is the compulsive need to pick that lands this particular disorder in with other obsessive-compulsive and related disorders.
Medical reviewers have even found that those who suffer from skin-picking disorder are more likely to also have OCD compared to those without.
You can be a skin picker without OCD
For those with skin-picking disorder, the act of excessively picking skin is often done to alleviate the constant urge to pick or touch the skin.
Similar tools are used with sufferers of OCD in that compulsive and ritualistic behavior is used to diffuse the uncertainty and anxiety felt by obsessive thoughts.
However, a skin-picking disorder focuses purely on picking scabs, spots, and scars, and can occur without comorbid OCD. You can receive an excoriation diagnosis without also receiving an OCD diagnosis.
With OCD, there is a wider range of compulsive ritualistic behaviors as a result of intrusive and obsessive thoughts. For example, some compulsive rituals might include:
The urge to pick may be an obsessive-compulsive behavior but it is not, in isolation, a symptom of OCD.
When does skin picking become a problem?
Skin picking becomes a problem when it begins to affect your daily life.
If skin-picking behavior gets to the point that it is near-constant, affecting your ability to see friends or carry out your responsibilities at work and school, this may be the time to seek a medical assessment to see if you are dealing with excoriation disorder.
Someone with a skin-picking disorder can develop damage to areas of their body that are easily seen by those around them. Scars and skin damage to the face are incredibly common and can leave the sufferer feeling embarrassed and ashamed.
This is not a disorder to be taken lightly despite how minor it may appear to someone with little knowledge of the condition.
While people with dermatillomania may not want to stop picking their skin, they don’t like the consequences of doing so and they feel very controlled by these urges. They feel as though they have little control over this strong urge and they feel like they have to pick.
There’s a reason that disorders such as this are often accompanied by high levels of anxiety, stress, and depression. It’s because it can be psychologically and emotionally difficult to manage day-to-day life.
It’s important to know that skin picking can be treated and managed so if you suspect you might be struggling with this condition, seek appropriate support from a mental health professional.
Both OCD and excoriation disorder – together or separately – can be treated effectively.
The ABC’s of Skin Picking
OCDLA created a simple and clear classification of dermatillomania to help us understand when skin picking becomes a problem. Because let’s face it, we all pick! But when does it start to matter?
“A” is something almost anyone would pick.
Something that anyone would feel inclined to pick might be some dry skin hanging from your arm or elbow, a scab that’s mostly fallen off, or a full spot on your chin that’s ready to burst!
“B” is a bump, pimple, or scab.
This is something that only a skin picker would pick at. At this stage, there is very little there to actually pick unlike the things noted in the “A” category. But a skin picker may feel for little bumps or potential spots and begin to pick.
Everything in the “B” category has the potential to turn into something from the “A” category or would disappear if left alone. But a skin picker will pick at these things and make them worse which ultimately causes high levels of distress and skin damage.
Those with skin-picking disorder may contribute at least 50% of their skin-picking to this category.
“C” stands for create.
Only someone with dermatillomania will find themself in band C. In this category, the sufferer does not pick at anything real per se, they pick at seemingly healthy skin and therefore create something such as a cut or blemish that was not there before.
In this category, the picker does not pick at anything apparent on their skin. Instead, they create skin damage through the act of picking at healthy skin.
What are the causes of skin picking?
Photo Credit: Engen Akyurt
The exact causes of excoriation disorder, like causes of OCD, are unknown. But there are a few factors that can trigger people to pick at their skin.
Boredom
Stress
Anxiety
Feelings of guilt or shame
Acne or eczema (skin lesions)
There may be a spot or scab that is deemed unsightly that the person wants to remove
Research suggests that the disorder may be linked to genetics. A study from 2012 found that out of 60 people with excoriation disorder, 28.3% had close family members who shared the same disorder.
(OCD) and body dysmorphic disorder (BDD), two types of obsessive-compulsive and related disorders, are also more common in people with skin picking disorder than in those without the disorder.
Research figures highlight that 28% of those with BDD also have excoriation or skin-picking disorder.
Two types of skin picking:
Automatic: This type of skin picking is more habitual and can be done without a person knowing they’re even doing it. Within this type of skin picking, the person may be seen running their fingers over their skin to check for any areas that feel different and could be a focus area for skin picking. This behavior is also known as ‘scanning’ and can be described as being in a trance-like state. In this trance-like state, they can lose track of time completely and fall into trance-like behaviors when they are picking.
Focused: This type of skin picking is more intentional, and an episode can last four extended periods of time, leading to greater skin damage.
There are several symptoms of skin-picking disorder:
Excessive and compulsive picking
Picking to the point of skin damage – being required
Digging into the skin using fingers, tweezers, knives, teeth, etc.
Common areas of focus such as the face where acne may be present are typical, and moles or freckles are targeted in an attempt to remove what is considered a blemish.
People with skin picking disorder will exhibit behaviors absent-mindedly, scanning for areas without much thought, but they can also have focused “sessions” where specific areas are targeted with picking lasting for hours at a time.
This is the more severe behavior trait and in some cases can result in surgery.
Diagnosis of skin-picking disorder
Source: Diana Polekhina
Diagnosing excoriation disorder requires a physical exam from a healthcare professional and some questions about any skin-picking behaviors to try and figure out if a skin-picking habit has crossed into a disorder.
Diagnosing this condition requires meeting all five of thefollowing criteria:
Recurrent skin picking that damages the skin.
Repeated attempts to stop or to do it less often.
Detrimental impact on various aspects of your life because of shame or embarrassment due to skin picking.
Skin-picking behavior occurs without the influence of any other medical condition such as scabies, eczema, acne, or drug use, whether recreational or prescription.
Picking isn’t the result of another mental health condition, such as body dysmorphic disorder, where you believe that you have a perceived physical defect that impacts your sense of self-worth and self-confidence so you pick at your skin to relieve those negative feelings.
Treatment for OCD
Source: Brooke Cagle
OCD is a long-term condition and the treatment for OCD will reflect this. The most effective treatments are psychotherapy and medication.
Psychotherapy
Cognitive behavioral therapy or CBT is used for many psychological problems, including OCD. Exposure and response prevention (ERP), is a type of CBT that involves gradual exposure to obsessions while resisting the urge to perform compulsive behaviors as a coping tool. The aim is to help teach your brain that you are capable of managing anxiety and uncertainty without the use of these coping mechanisms.
Medication
Antidepressants known as selective serotonin reuptake inhibitors (SSRIs) are designed to increase the levels of serotonin in the brain. These are often prescribed alongside psychotherapy.
Medication should only be taken if prescribed by a mental health professional. Please seek medical assistance and effective medication treatment that is tailored to you and your needs.
Treatment for excoriation disorder
Source: Andre Hunter
Medication isn’t used to treat excoriation disorder, treating skin-picking disorder follows two main kinds of psychotherapy…
As with OCD, CBT has been shown to be effective at treating excoriation disorder by helping to change how their relationship and response to stressful or overly emotional situations. More specifically, a technique called habit reversal training is used to help identify what causes these urges and develop alternative, less harmful behaviors.
Making changes to your surroundings and limiting the opportunity to act on urges to pick is also effective.
This is known as stimulus control and a therapist will work with you to make it harder to act on these urges. Wearing gloves or band-aids can help by reducing the opportunities to pick and other changes, such as removing mirrors or covering reflective surfaces, limits exposure to face acne or other blemishes that may usually trigger the urge to pick.
Trichotillomania – also known as the ‘hair-pulling’ disorder – is categorized as the repetitive and uncontrollable urge to pull hair from your body. While some confuse it with OCD, it is in fact a separate condition.
While hair can be pulled from any part of your body with this condition the most common areas include the scalp, eyelashes, eyebrows, arms, pubic hair, and armpits.
Hair pulling is a real mental health condition and can lead to feelings of low self-esteem and a lack of self-confidence.
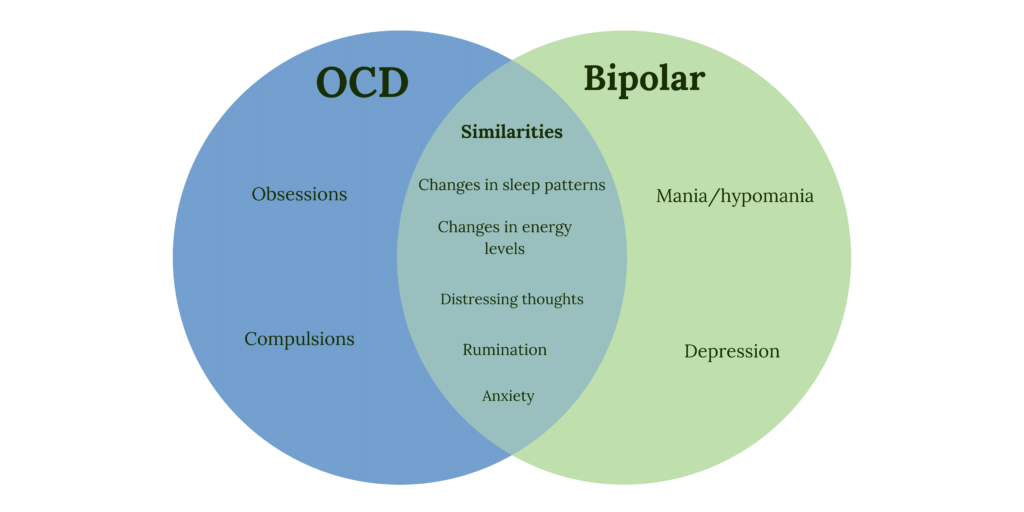
Obsessive-compulsive disorder (OCD) and bipolar disorder share many symptoms but there is also a key distinction between the two.
OCD is an anxiety disorder characterized by disturbing and unwanted obsessions in the form of thoughts, images, urges, feelings, or sensations. This is followed by repetitive ritualistic behaviors done with the aim to alleviate the uncertainty and anxiety caused by these obsessions.
Bipolar disorder is a mood disorder that is characterized by extreme changes in mood, thoughts, and behavior.
The relationship between the two has been the subject of numerous studies and research carried out in 2015 found that those with bipolar disorder are more likely to exhibit symptoms of OCD, compared to those with no diagnosed mental health illness.
This does not mean that having one guarantees you will have the other.
However, the statistics show that anywhere up to 20% of those living with bipolar show lifetime comorbidity with OCD.
In order to receive accurate medical advice, diagnosis, or treatment, it is important to first identify the characteristics of each.
What is OCD? A Brief Overview
Photo Credit: Brooke Cagle
There are two core components of OCD, obsessions, and compulsions.
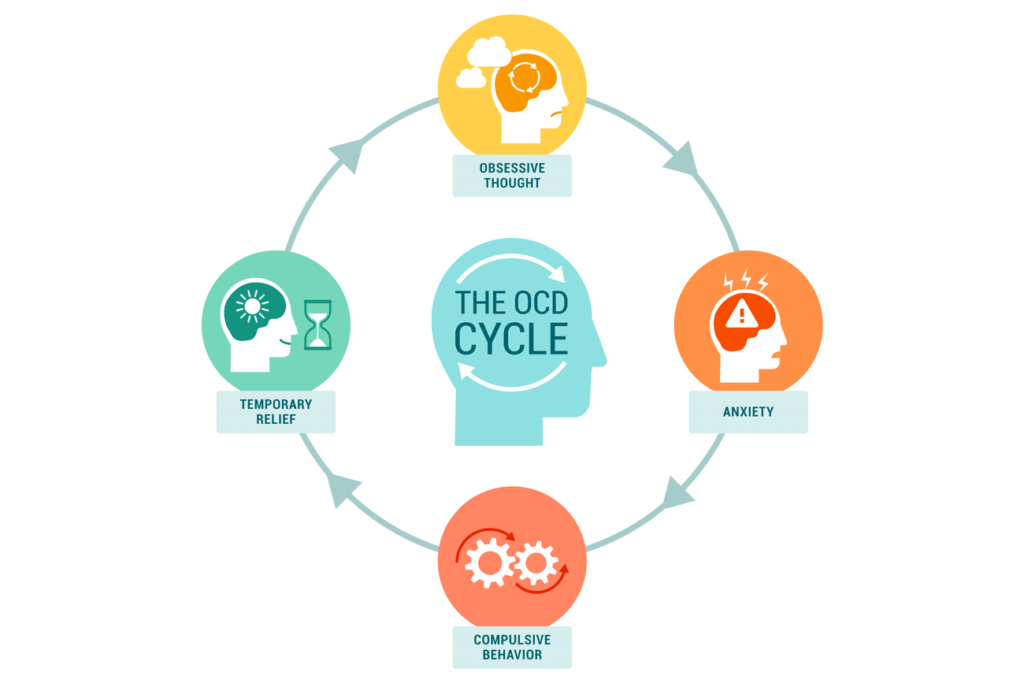
The OCD cycle begins when the sufferer is triggered by an obsession and intrusive thoughts. These obsessions are very sticky and difficult to shake for an OCD sufferer precisely because they go against their values.
When those obsessions arise, the sufferer feels the need for certainty.
Instead, they doubt themselves. They can find themselves trapped in a loop of rumination:
Why did I think this thought?
What does this mean about me?
What will happen if I don’t do something about it?
How can I be sure it isn’t true?
These intrusive thoughts can be torturous and painful to live with for someone with OCD. This is why the sufferer then engages in compulsions.
Compulsions are the repetitive, ritualistic behaviors we then do in order to gain some sense of certainty (if only for a short while) and find relief from the anxiety.
The most overplayed representation of OCD in pop culture and media is the need to excessively wash hands or clean. But there are a vast array of subtypes that cover a great deal of context beyond contamination OCD – there is simply a lack of education and understanding at this time (although that’s changing!).
It is often difficult for those not suffering from OCD to recognize the link that a compulsive action has to an intrusive thought and not all compulsions are visible to others.
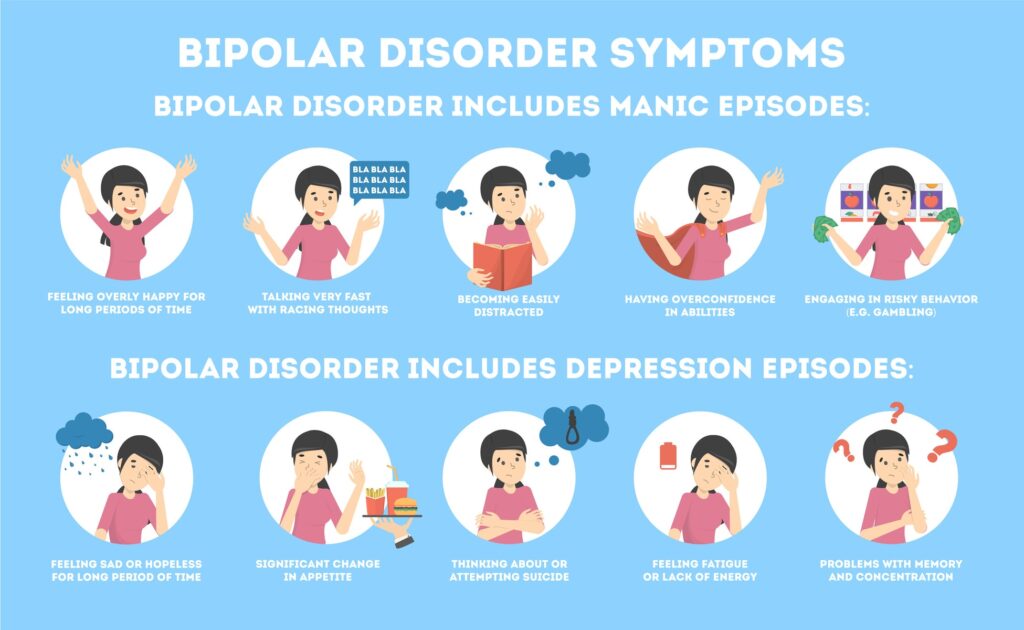
Bipolar disorder is a chronic mood disorder that causes sufferers to experience severe changes in mood, activity levels, energy, and concentration.
People with bipolar disorder will have emotional highs (mania) where they experience feelings of extreme euphoria. And in contrast, extreme emotional lows leave them feeling lethargic, sad, and oftentimes, hopeless.
The severe shift in mood is known as an episode.
As with all mood disorders, an individual’s mood doesn’t necessarily match their circumstances and it will have a detrimental effect on a person’s ability to complete day-to-day functions.
Bipolar disorder is usually diagnosed in adolescence but it can occur at any age with symptoms varying over time and from person to person.
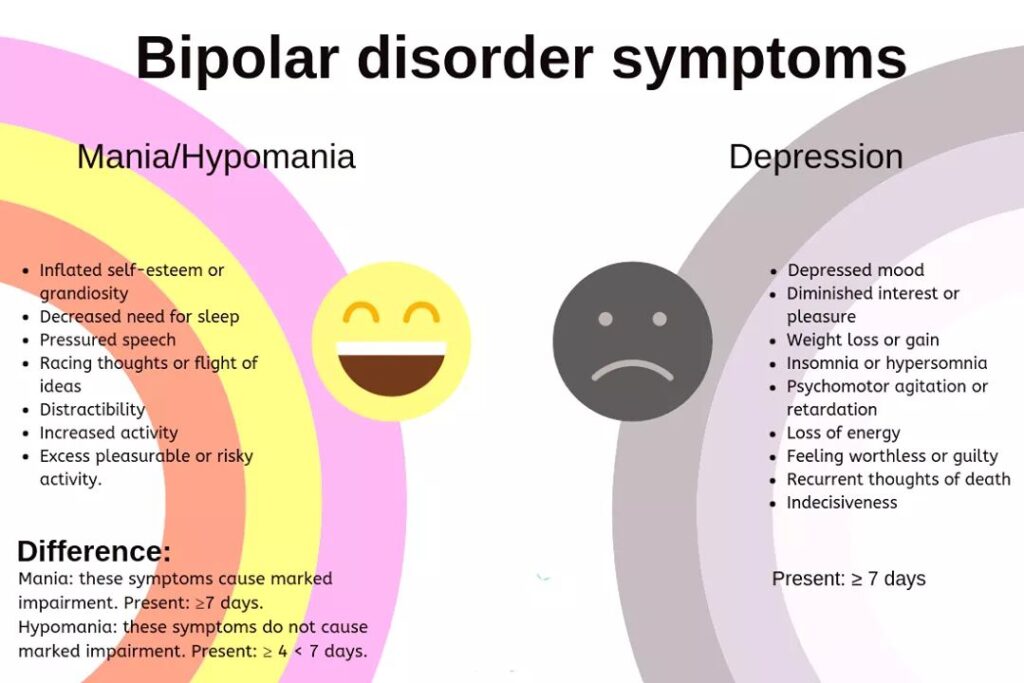
Mania/hypomania
Mania refers to an episode of extreme emotional highs that lasts for a week or more.
Hypomania is the milder of the two, lasting for only a few days and although the symptoms experienced are similar, hypomania is considered the more manageable of the two as the episodes are shorter-lived.
Although mania/hypomania represents the ‘highs’ of bipolar disorder, this isn’t to be confused with ‘feel-goods’. The highs are just as detrimental to a sufferer’s day-to-day life as the lows are.
Episodes of mania or hypomania can be identified by feelings of:
Uncontrollable excitement
Irritability
Increased sexual energy
Inflated self-esteem
Impulsivity
Experiencing these feelings during a manic episode leads to changes in behavior such as:
Sleeping less
Acting aggressively
Drug or alcohol abuse
Increased levels of activity
Reckless decision-making that puts your safety at risk
Speaking much more quickly than normal
Acting out of character
Reckless purchases or money spending
Depression
The contrast to mania and hypomania is depression.
Depressive episodes can last anywhere from a couple of weeks to months at a time and are as equally disruptive as the mania.
The swing from high to low moods can be considerably jarring and leave the sufferer feeling like they have no control.
Depressive episodes leave individuals feeling:
Sad, hopeless, and dejected
Lethargic or low-energy
Uninterested in anything
Worthless
Unable to concentrate
Lacking in confidence
Anxious
Suicidal
The behavioral changes might look as follows:
Shying away from social situations
Ignoring friends
Changes in sleep patterns
Eating too much or not enough
Less physically active
Rumination (repeatedly focusing on negative thoughts)
Drug or alcohol misuse
Attempts to self-harm or attempt suicide
Mixed episodes
These episodes of mania/hypomania and depression can shift very quickly from one to the other or even occur at the same time. This results in unpredictable behavior and confusion, not only in its sufferers but for those around them.
Feeling recklessly impulsive and confident while hopelessly dejected can be difficult to explain and may cause individuals to act erratically.
Mixed episodes can also last from weeks to months and the prevailing evidence from medical reviewers shows that those who suffer mixed episodes are at a greater risk of attempting suicide compared to those who suffer episodes in isolation.
Bipolar disorder is broken down into multiple categories for diagnosis:
Bipolar 1 – at least one episode of mania lasting longer than a week. This can be preceded or followed by hypomanic or depressive episodes.
Bipolar 2 – at least one episode of depression and hypomania but not mania.
Cyclothymia – an experience of multiple hypomanic and depressive episodes over a two-year period although the severity of the symptoms does not meet the criteria to be considered bipolar 1 or bipolar 2. When diagnosing teenagers, the period of time required is reduced to one year.
‘Other’ – This diagnosis is reached if symptoms do not fit into any of the above or if they are experienced alongside other medical conditions.
Shared symptoms of OCD and bipolar disorder
The symptoms shared by both OCD and bipolar disorder include:
Changes in energy levels
Changes to sleep patterns
Erratic and sudden mood swings
Rumination (repetitive negative thoughts during a depressive episode)
The strain on both home and work life
Distressing thoughts
Anxiety
Some symptoms of depression
There is a clear overlap and someone with OCD can exhibit symptoms of bipolar disorder without a specific bipolar disorder diagnosis (and vice versa), though these may only be experienced during periods of mania or depression.
Differing symptoms
Symptoms that are caused by OCD but not bipolar disorder include:
Obsessions – For example, someone who has intrusive repetitive thoughts may be up all night, crying, unable to leave the house, fearful of what might happen if (insert fear)… This is a symptom of OCD, not bipolar disorder.
Compulsions – For example, someone may engage in repetitive behaviors such as repetitive checking, reassurance seeking, or staring compulsions. This could appear to be a manic episode to the untrained eye, but it is in fact a symptom of OCD.
Symptoms that are caused by bipolar disorder but not OCD include:
Mania/hypomania – Even though people with OCD have good days and bad days, this is not the same as a manic episode experienced by those with bipolar disorder.
Depression – Likewise, it is very common for someone to live with OCD and depression. OCD is a very difficult disorder to live with and can lead to periods of hopelessness. This is also quite different from a depressive episode experienced by someone with bipolar. This is why it’s so important to receive the correct diagnosis because many confuse the two but they are very different.
Psychosis (in certain cases)
To the untrained eye, a person suffering from obsessions and compulsions associated with OCD may appear to be having a bipolar episode. However, this is why it’s very important to receive a thorough assessment so that you can are treatment for the correct disorder.
If someone with OCD is having racing intrusive thoughts or performing repetitive ritualistic compulsions, it can be common for them to be misunderstood as having bipolar disorder.
If you suspect yourself of having one or the other, or both, you must be thoroughly assessed so that an appropriate treatment plan can be made for you. For someone living with both OCD and bipolar disorder, it is imperative that their bipolar be treated before they begin treatment for OCD as it will affect their OCD recovery.
If you feel like your symptoms are better understood as obsessions and compulsions and you would like to have a thorough assessment from someone from our team to receive the correct diagnosis and treatment, please submit a submission form HERE(for those based in California).
What is it like living with both disorders?
Photo Credit: Tengyart
Living with OCD or bipolar disorder independently from each other can be challenging. If you are experiencing both it may bring some additional challenges.
It is completely understandable, therefore, that someone would feel overwhelmed when faced with a life of both.
The good news is there are science-based treatment modalities for both OCD and Bipolar disorder. Thanks to many years of research, we also have medications that are proving to be highly effective for those managing both OCD and Bipolar disorder.
Please speak with your medical professionals to determine a medication plan that will be helpful for you.
The more knowledge and understanding you have, the better equipped you will be to manage both.
How OCD impacts bipolar symptoms
OCD symptoms can exacerbate depressive episodes and increase the severity of bipolar symptoms.
The fear and uncertainty triggered by those obsessions can, during a bipolar depressive episode, only add to the feelings of hopelessness and despair felt by the sufferer. It feels like another thing to manage and another thing that they don’t feel able to deal with.
The uncertainty and self-doubt that arise during the OCD cycle contribute to great doubt and uncertainty surrounding bipolar symptoms.
Rumination (repetitive and unhelpful ‘problem-solving’ thoughts) is a symptom of each and when experienced as a result of OCD, it can cross over and latch on to bipolar symptoms as well.
It is essential that the person with bipolar has been assessed by a medical professional to make sure the symptoms of bipolar disorder are treated before they begin treatment for OCD.
How bipolar impacts OCD symptoms
During a depressive episode brought on by bipolar disorder, negative thoughts and low emotions as a result of OCD are increased.
Anxiety levels are also heightened with the introduction of bipolar disorder which can lead to increased obsessive thoughts and subsequent compulsions.
That said, there is evidence to suggest checking compulsions are reduced compared to someone with OCD in isolation and theories suggest that OCD symptoms are less severe during mania/hypomania episodes and heighten during depressive episodes.
Are OCD and Bipolar connected?
Photo Credit: Joann Boyer
Currently, scientists are not sure where the connection lies between the two conditions. However, there are some things that we can consider…
Genetics: Like OCD, there could be a genetic factor involved in the onset of bipolar disorder. Research suggests that there are a number of genes shared by both disorders. While this is not definitive, it is something that researchers continue to explore.
Intrusive thoughts and obsessive thinking: Intrusive thoughts and some form of negative obsessive thinking feature heavily in both disorders and this could be down to a commonality between the two.
Anxiety: As with obsessive thinking, anxiety and anxious thoughts appear with both conditions. This could also be a commonality that connects the two conditions.
When you’re in the middle of living with not only one condition but two simultaneously, it’s not difficult to see why someone may begin to lose hope. But there is hope. The saving grace is that extensive research has been conducted on the most effective treatment for OCD and bipolar individually, as well as in co-occurrence.
Treatments for bipolar disorder
Treatment for bipolar disorder needs to be long-term. It is a chronic illness and should therefore be carried out even during episode-free periods.
Medication
Mood stabilizers will typically be introduced to control symptoms fast and are sometimes used in conjunction with other medication to be most effective.
Antidepressants can sometimes be used as a medication for bipolar disorder however, in many cases they contribute to cases of mania and hypomania. Because of this, certain mood stabilizers tend to be the first option.
This should not be taken as medication advice, please speak to your medical professional to receive the appropriate medication plan for you.
Psychotherapy
A form of talking therapy will take place alongside the use of mood stabilizers. The type of therapy will depend on what best suits you and your needs. There are many different types of psychotherapy available, including:
Psychoeducation is designed to teach your condition so that you are better placed to identify triggers.
Cognitive behavioral therapy (CBT) helps with the management of symptoms by helping you identify negative thoughts and behavioral patterns.
Interpersonal therapy is designed to highlight how your thoughts and behavior impact your relationships with other people and the effect those relationships have on you in return.
Treatments for OCD
As with bipolar disorder, Treatments for OCD need to be long-term to reflect the long-term nature of the condition.
Psychotherapy
Cognitive Behavioral Therapy (CBT) is used for many psychological problems, including OCD. Exposure and response prevention (ERP), a type of CBT, involves the gradual exposure to obsessions whilst resisting the urge to engage in compulsive behaviors as a coping tool. This method of treatment is designed to help you change your relationships and respond to those obsessions.
Medication
Typically a form of antidepressant known as selective serotonin reuptake inhibitors (SSRIs) are shown to be helpful when prescribed alongside psychotherapy.
Medication should only be taken if prescribed by a mental health professional.
Treatment for both together
The treatment of bipolar disorder takes precedence when both disorders are being treated together. It’s important that a person’s mood is stabilized before treatment for OCD begins. This follows research suggesting OCD treatment is ineffective if symptoms of bipolar disorder are not dealt with first.
The psychological treatments listed above for each disorder remain effective but due to the heightened risk of substance abuse, self-harm, and erratic behavior in those diagnosed with both, closer monitoring is required.
It is important to ensure that you seek assistance from a specialist who is highly qualified in both disorders, as having the two together can contribute to complications in therapy if you aren’t under the correct guidance.
We have a qualified team of elite clinicians based in California, who can assess and treat OCD. We are able to rule out Bipolar disorder however if you have additional bipolar symptoms we would refer you to specialists who come highly recommended in the treatment of Bipolar disorder.
We will be able to treat your OCD in conjunction with any other bipolar treatment you receive elsewhere.
If you would like to see how we might be able to help you with an appropriate assessment, please submit an inquiry form here.
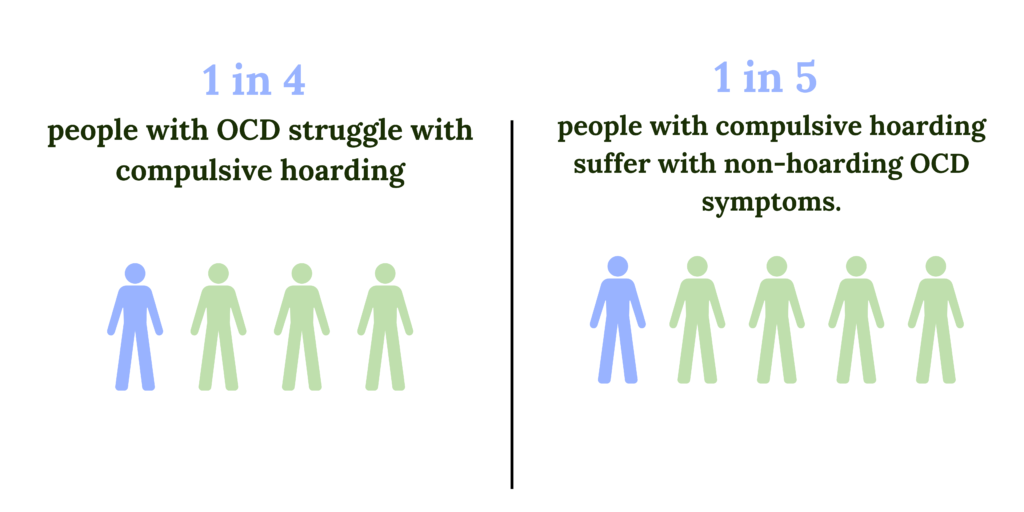
Compulsive hoarding used to be considered a type of OCD.
Some have estimated that up to 1 in 4 with OCD also struggle with compulsive hoarding. And up to 1 in 5 compulsive hoarders have non-hoarding OCD symptoms.
Like many other comorbidities (such as OCD and depression, or OCD and BDD), there is a distinct overlap between the two disorders.
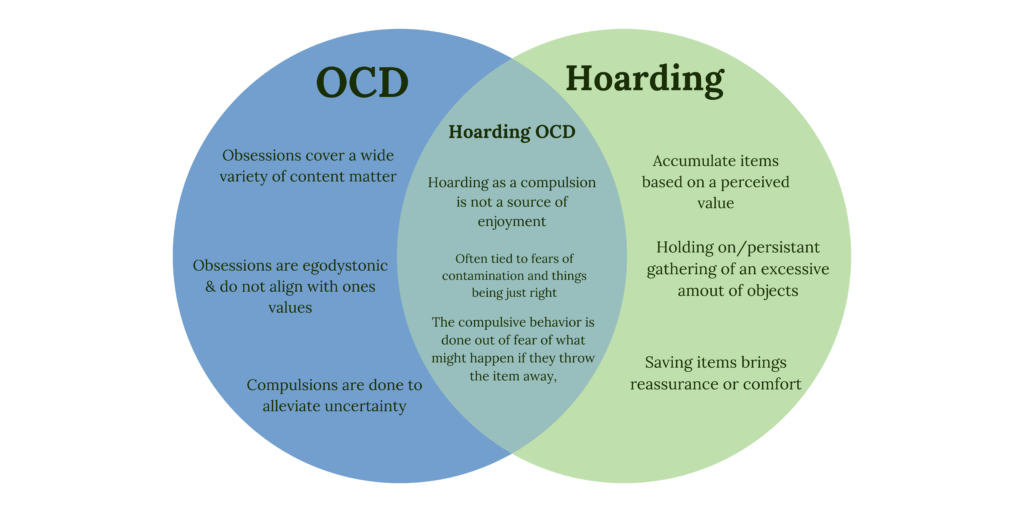
You can be diagnosed with hoarding disorder without an OCD diagnosis. A hoarding disorder with an OCD diagnosis is known as hoarding OCD.
Like many OCD subtypes (and mental health disorders in general) hoarding and hoarding OCD are greatly misunderstood. Both hoarding and hoarding OCD are great sources of pain and stress; they are not enjoyable and they do not bring pleasure to one’s life.
It can have a huge impact on quality of life which, to those who do not understand the disorder, can appear as a way of living that the sufferer may even enjoy.
This is simply not true.
Let’s look at OCD and hoarding separately and together to understand the differences between the two.
OCD: A Recap
Photo Credit: Marina Vitale
People with OCD will suffer from obsessions in the form of thoughts, images, feelings, urges, or sensations. Intrusive thoughts will pop into their head, causing an immense amount of stress and discomfort.
These unwanted and intrusive thoughts are disturbing or fearful in nature and conjure tortuous feelings of uncertainty and distress.
These intrusive thoughts are constant, persistent, and all-consuming and the sufferer will try desperately to alleviate their distress.
This distress leads to a physical or mental compulsion; a ritualistic behavior aimed at soothing the anxiety and uncertainty brought on by distressing thoughts.
Anxiety felt around any uncertainty and thoughts of “what if?” brings with it cravings and urges for certainty.
We do compulsions to try to solve that uncertainty and mitigate any potential consequences of not addressing the obsessions.
In doing this, our brain learns that the physical or mental ritual is needed in order to navigate the uncertainty and anxiety. We learn that we cannot tolerate those feelings without doing compulsive behaviors.
But, the relief this offers is only fleeting and allows OCD to thrive. This is known as the OCD cycle and it acts to perpetuate long-term feelings of distress.
Click here to sign up for our weekly newsletter and receive immediate access to the 6-part mental compulsions audio series to help you resist the urge to engage in mental rituals (PDF worksheets included)
What is hoarding
Photo Credit: Dim Hou
Hoarding is characterized by the persistent gathering and saving of an excessive number of objects. The ‘excessive’ part comes into play as the sheer volume is unmanageable, storage is chaotic and the behavior has a detrimental effect on everyday life.
The items will likely have no monetary value and will create clutter to the point that access to a person’s home is compromised.
People who experience hoarding feel greatly distressed at the thought of discarding the items they have hoarded.
When is hoarding considered a problem?
Hoarding is considered a problem when:
It starts to affect someone’s ability to look after themselves or their family. For example, if access to the kitchen or cooker is blocked, individuals with hoarding disorder will stop feeding themselves or their families properly, choosing to work around the clutter by skipping meals or eating out, despite sometimes not having the financial resources to do so.
The idea of parting ways with the clutter brings on significant distress. They can become upset if someone tries to tidy up or remove items and this can have an adverse effect on relationships.
People who struggle with hoarding can also find themselves isolated from friends or family, and be unwilling to have anyone else enter their homes.
In extreme cases of hoarding, an individual’s safety is at risk as fire and tripping hazards are littered about their home.
They believe these items will be needed at some point in the future
They have ‘a great find’ believing the item to be unique and interesting
The items have significant sentimental value, representing a lost loved one or a previous time in their life that brought great joy
The things that they save bring reassurance or comfort
The thought of missing out on the opportunity to benefit from the items is distressing
Often, someone with hoarding OCD has a fear of contamination.
Contamination fears are not the only type of obsession in hoarding OCD, but it is very common.
The difference between hoarding and collecting
Photo Credit: Karen Vardazaryan
Collectors will typically take great joy in organizing or filing their collection for admiration.
The presentation will be neat – think stamps in a scrapbook – and the collection will be carefully considered and follow a theme. Collections can be large but they are not disorderly and their existence does cause a detrimental effect on lives.
Hoarding is impulsive and follows no discernible theme. Presentation, in order to admire, isn’t considered and the clutter can often be a source of embarrassment or shame.
A collector will have the presence of mind to budget money and space for their items, whereas the impulsivity of individuals with hoarding disorder means that their items can cause financial strain or debt.
Signs of hoarding disorder
Here are some key signs to look out for when identifying hoarding disorder:
An individual’s home, car, or office space is so cluttered that it is difficult to navigate
Storage units are rented to accommodate the sheer volume of possessions
The individual flat-out refuses or has difficulty discardingpossessions
Discussing the removal of cluttered items is met with dismissive or aggressive behavior due to anxiety
The individual struggles with the organization and order of their possessions
Showing signs of shame over the amount of clutter in their home
Overly possessive feelings towards their possessions, i.e. an individual won’t allow others to touch their things
Signs of obsessive thoughts and behavior towards items such as looking through trash or showing distress when they believe something has been disposed of.
Feeling overwhelmed at the amount of clutter and feelings of deep shame
In extreme cases, a hoarding disorder will inhibit someone’s ability to work, take pride in their appearance, and have financial stability and it will affect relationships with friends and family.
Wanting to save items for fear of needing them at a later date but then, when the time comes that they need the item they can’t even find it.
Difference between hoarding disorder and hoarding OCD
The best way to differentiate between hoarding OCD and hoarding disorder comes down to the reason why the sufferer is hoarding.
For a long time, hoarding disorder was considered to be a part of OCD. In recent years, hoarding disorder has been given its own diagnosis and what separates the two is mainly down to the reasons for the compulsive behavior.
Individuals with hoarding disorder accumulate items because they perceive them to be valuable, and unique or believe that one day they will have a use for them.
Distress is experienced when faced with the prospect of throwing possessions away because of this perceived value.
Whereas hoarding OCD is an unwanted behavior done in response to an obsessive thought.
For those with hoarding OCD, the accumulation and retention of objects are often very stressful as they find themselves ruminating on the potential consequences of what might happen if they were to get rid of said items.
A helpful distinction between hoarding OCD and hoarding disorder is that those with hoarding disorder hang on to items they feel are valuable and feel distressed at the idea of getting rid of them. Whereas hoarding OCD, people are holding onto items because they fear what will happen if they don’t.
Example of hoarding OCD obsessions
Hoarding OCD obsessions could sound like:
I need to buy six of these cans of soup as the labels match up with those I already have at home and these six cans will fit perfectly in the cupboard
I don’t need this sweater anymore and should donate it to a thrift shop, but they might be contaminated and I don’t want to make anyone ill
I should throw out these plates but what if they break in the bin and someone cuts themselves on the sharp edges?
The trash has been sitting by the door for ages now but I don’t want to touch the outside garbage bin in case I catch anything that could make me ill
These wedding favors were left by the guests after our wedding. I’ll hold onto them in case throwing them away is a bad omen
I need to keep this because it feels wrong to get rid of it/this item feels right to keep.
I see other people are throwing this out and doing so damages the environment so I have to keep this to save the planet.
Examples of hoarding OCD compulsions
Hoarding compulsions might look like:
Waiting until the same register clerk is available to scan your groceries
Purchasing items in specific sets, i.e. only ever three bananas, only ever six cans at a time, two cartons of milk even though there is only the need for one
Purchasing items that have been touched, even if you don’t want/need them
Storing dirty items in a specific drawer or cabinet for fear of contamination
Keeping hold of items that could be considered ‘trash’
ERP therapy for Hoarding OCD
Photo Credit: Angel Balashev
Cognitive behavioral therapy (CBT) with exposure response prevention (ERP), is the gold-standard treatment for OCD disorders, including hoarding OCD.
Through repeated exposure to obsessive thoughts, wilfully tolerating the anxiety and uncertainty, and resisting the urge to do compulsions (hoarding in this instance) we teach our brain that we are capable of navigating the uncertainty without those safety behaviors.
Falling into an OCD cycle is all too easy but by changing our response to those obsessions we provide our brains with new tools that can be used to soothe our anxieties, away from the detrimental and compulsive behavior we may have exhibited in the past.
ERP exposures for hoarding OCD
ERP works by gradually exposing yourself to your obsessions and taking small steps toward changing how you think and behave toward them.
With hoarding OCD in mind, you will work closely with your therapist to break away from your compulsions, for example, going to a grocery store and only buying one item instead of multiples.
With your therapist, you’ll first come up with a hierarchy of exposures you are willing to do and be given education on how to reduce compulsions such as mental compulsions, avoidance compulsions, reassurance compulsions, and hoarding compulsions.
You will also discuss your feared outcome and address ways in which you can expose yourself to those fears.
Along with exposure to only accumulating one item at a time, the therapist and client will also work at exposing the client to getting rid of the hoarded items in the house. This is done in a step-by-step manner where the client themselves get to choose what they are willing to get rid of.
When the degree of clutter is so much, the client and therapist may consider the option of hiring cleaners to discard the items to help the client maintain a degree of safety in their home, if they are unable to do it at a pace that reduces the safety risk.
The aim is to become more comfortable with obsessive thoughts, to identify them, and break away from the compulsive, ritualistic behavior that follows.
If we familiarize ourselves with uncertainty and discomfort, we’re far less likely to fear it. And if we no longer feel apprehensive in the face of the unknown, we’re far more likely to live full and satisfying lives.
People with obsessive-compulsive disorder (OCD) and body dysmorphic disorder (BDD) exhibit many similar symptoms to the extent that BDD has, for a long time, been labeled as a form of OCD.
While they are both anxiety disorders, they are quite different.
OCD is a common mental illness affecting up to 2% of the world’s population. What many people don’t know, is that it is not unusual to live with OCD and other related disorders simultaneously. OCD and depression are two mental health conditions that often go hand in hand.