False Memory OCD (Obsessive-Compulsive Disorder) is a subtype of OCD that involves recurrent, persistent, and intrusive thoughts or doubts about past events or experiences.
These thoughts or doubts are often accompanied by strong feelings of guilt, shame, and anxiety about the experience, even when the person with OCD cannot be sure that the thoughts are rational or true.
In False Memory OCD, a person may obsess over a memory or a thought that they believe is a true event from their past, but in reality, the memory is false or distorted.
Sexual orientation OCD (SO-OCD) is an OCD subtype that is characterized by immense fears about an individual’s sexual orientation.
This subtype was originally referred to as HOCD (homosexual OCD), but SO-OCD affects people of all sexual orientations. HOCD is now only used to describe those who very specifically struggle with homosexual obsessions.
Those with SO-OCD are plagued with highly distressing intrusive thoughts and urges that make them doubt their true sexual orientation.
Suicidal obsessive-compulsive disorder is categorized by the terrifying and unwanted fears about killing oneself.
Closely linked to Harm OCD, this subtype is sometimes called harm OCD with suicidal obsessions. Although the fears of potentially harming oneself feel very real, suicidal OCD is actually driven by the desire to protect oneself from harm.
Those with this subtype are no more likely to die by suicide than any other OCD subtype.
Harm OCD is a subtype of OCD that focuses on obsessions surrounding harm to self and/or harm to others.
For people with OCD, harm thoughts evoke excessive feelings of shame due to the violent nature of the intrusive thoughts and the misunderstanding of OCD. It is important that you understand that there is nothing to be ashamed of.
Harm obsessions can be all-consuming fears about our own safety or the safety of the people that the sufferer loves most.
Emetophobia is the intense fear of vomiting. For those with this specific phobia, extreme fears surround the thought of vomiting, seeing other people vomit, or feeling nauseous.
For those suffering from this disorder, it goes beyond a typical response of disgust toward vomit (after all, who doesn’t recoil a little at the sight of it?). People with emetophobia actually fear it.
To the untrained eye, symptoms of emetophobia and OCD overlap so much that one could easily be mistaken for the other.
Fear of choking is known as pseudodysphagia, often confused with phagophobia which is the intense fear of swallowing.
The two commonly overlap but you can experience one without the other.
The difference is small but distinct. Those with phagophobia fear the process of swallowing, while those with pseudodysphagia are afraid of choking after swallowing.
Choking phobia is a rare condition where sufferers hyperfocus on the sensations they experience when eating and swallowing food in a desperate bid to avoid choking at all costs.
Avoidance becomes a dominant behavior in this cycle. People with choking disorder may restrict their diet and avoid certain food types, blend their food to reduce the risk of choking, and may also avoid taking tablets.
Fear of choking within OCD involves the intense fixation on the bodily sensations when swallowing, with a particular focus on the back of the throat. The vicious cycle sufferers find themselves trapped in remains the same; caught in a loop of obsessions, uncertainty, and compulsions.
Fear of choking within OCD
Diagnostically, the fear of choking (pseudodysphoria) is categorized as a Specific Phobia and lands in the category of specific phobia disorder of anxiety disorders in DSM IV, and has been retained in DSM 5 (The Diagnostic and Statistical Manual of Mental Illnesses).
Phobias often fall under a category called OCD spectrum disorders along with other conditions such as panic disorders and health anxiety, for example. All OCD spectrum disorders feature obsessions and compulsions.
Using the conceptualization of OCD, the fear of choking is the core obsession for someone with pseudodysphoria.
Those intrusive thoughts do not pass quickly, they are relentless and demand time and energy. Mentally, it’s exhausting. You can be left feeling trapped in loop of rumination about what might happen at the next mealtime, or how you’re going to manage at the next family birthday dinner.
The most common compulsion is avoidance behaviors and mental rumination. Most often, this looks like avoidance of certain foods (and drinks) because ultimately, those obsessions play on a fear that goes beyond choking; a fear of dying.
Because of this, it can result in malnourishment and have a negative impact on our physical health. People who suffer from this rare condition not only have to battle with the noise inside their minds but the medical implications as well.
Fortunately, like all phobias and anxiety disorders, it can be treated and you can feel free to enjoy the foods you love again and relieve yourself from the daily terror.
How does fear of choking present itself?
Obsessions:
Hyperfixation on the sensory feelings in the throat
Excessive fear of what might happen if they eat something without chewing enough
Hyperfixation on the texture of foods
Hyperawareness of sensations in the mouth and throat
Excessive fears about swallowing liquids, foods, or saliva
Compulsions:
Avoiding certain foods that ‘might’ cause you to choke, even if you love them
Avoiding going to the dentist for fear of the utensils they may use in your mouth
Ruminating about how you felt when you ate your last meal
Ruminating on how you’re going to cope at the next social gathering where food is a core component of the experience
Avoiding eating in front of anyone for fear of choking in front of them, or fear of judgment over what they might think of your eating/drinking habits
What does it feel like to live with a fear of choking?
Living with the fear of choking feels like constantly living on the edge of ‘danger’.
Every day we need to eat. Every day we need to ingest something at some point. We need to do this to stay alive, and so it’s tremendously debilitating to fear something that we have to face every single day.
People with a fear of choking can face challenges at every mealtime.
Battling with intrusive thoughts and ruminating on potential consequences, food becomes a source of angst and pain where it was once a source of joy.
The clients who come to work with us explain how they would love to love food again, instead of it being a trigger for their fears. Their fear of choking has them fixated on those bodily sensations in the back of the throat and food/drink (or anything that could cause us to choke) becomes the source of perceived danger.
Beyond this, pseudodysphoria can be incredibly isolating.
Many avoid social occasions where they know food or drink may be involved because they don’t want to have to wrestle with those fears in front of people.
What if they don’t understand?
What if I’m peer pressured into eating something I don’t want to eat?
What if they think my eating habits are strange?
It can become an incredibly lonely disorder, very quickly.
This mental health condition may be rare but it feels incredibly limiting and makes challenges out of behaviors we naturally do every single day.
If you resonate with this then the good news is that there are proven treatments that can help you get back to normality and stop this fear of choking from dictating how you choose to live your life.
Can OCD cause swallowing problems?
A common question clients have is whether or not OCD can cause swallowing problems.
OCD does not cause swallowing problems.
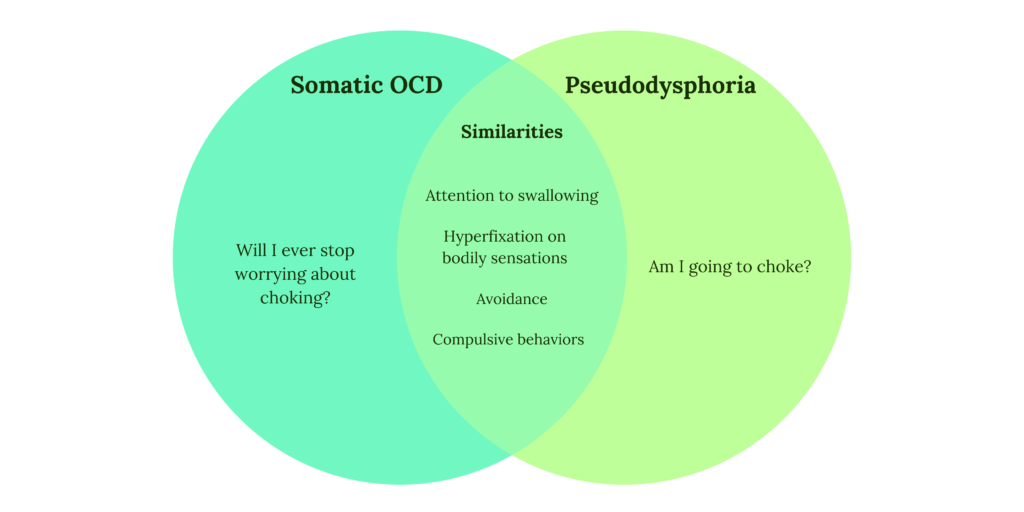
However, there is a subtype of OCD called Somatic OCD (or sensorimotor OCD) where sufferers fixate on swallowing and the frequency of swallowing.
Those with somatic OCD suffer from an intense fixation with their bodily functions. They may fixate on their breathing, blinking, or swallowing. For example, someone may wonder whether or not they are breathing too loudly or blinking too quickly.
In the case of pseudodysphoria, the focus is on the feelings and sensations within the mouth and back of the throat when swallowing.
But the fear is, ‘What if I choke on this and I can’t breathe?’
Whereas, for someone with Somatic OCD the fixation is “What if I never stop fixating on my swallowing?”
Someone who suffers with a fear of choking may find themselves caught in a catch-22…
When we are anxious about the uncertainty of whether or not we may choke on our next meal, tension arises in our throats. And because we’re hyperfocused on that area of our body – looking for any sign that something isn’t right and eating this food might be risky – we find it.
When you notice tightness in your throat, it does feel like something could get caught in there.
But because sufferers are now so aware of their bodily functions, any ‘sign’ becomes intensified.
When clients come to work with us, we work together to change the way we think and respond to those bodily functions in order to be free of this cycle and help regain a sense of control so that the client decides where they place their attention rather than the fear directing their attention.
What causes fear of choking?
It has been proposed that this mental health condition is most commonly triggered by traumatic experiences surrounding food and choking.
However, many clients come to us with a phobia of choking who have not had a traumatic experience like this.
The sufferer themselves may have choked on food at some point in their life, or may have witnessed someone else choking, or even seen it on a movie, for example.
Food (or ingestion of any kind) then becomes a trigger for anxiety.
The brain learns that anything that goes into our mouth is perceived as a potential source of danger. While our threat response is doing exactly what it should do – trying to protect us – disturbing thoughts about choking followed by paralyzing anxiety then incentivizes compulsive behaviors.
Although providing temporary relief, this then perpetuates the cycle of fear.
ERP therapy is a type of Cognitive Behavioral Therapy (CBT). It requires that you do these two things:
Return back to eating a wide variety of foods in multiple settings.
Choose a response other than avoidance or compulsive behavior.
This is an oversimplified overview of how the ERP process works, but ultimately, you will work together with your therapist to create a treatment plan involving exposures that are challenging but also achievable.
Together, you may look at the foods you avoid, for example, and begin to slowly reintroduce them into your diet.
The ERP process is gradual, so you will not be thrust into a situation that feels too big to handle. It’s not about throwing you into the deep end, it’s about taking small steps toward allowing yourself to be guided by your values rather than your fears.
We want to get you to a place where you can say, “What would I choose to do if I didn’t have this fear?” And do it!
It can feel scary to begin this process and many face resistance (which is entirely understandable – that’s fear talking!). However, when our clients begin working with us they rarely regret starting the recovery process.
There will be times of discomfort, but you face that discomfort with a cheerleader in your corner, knowing that it’s leaning into that discomfort that will allow you to live a life without limits once again.
Finding a qualified therapist
If this resonates with you, and you suspect you may be exhibiting symptoms of pseudodysphoria, then please reach out to our friendly team of highly qualified mental health professionals.
Based in the state of California, we are an elite team of trained clinicians who advocate for a compassionate and non-judgemental approach to mental illness recovery.
We’re here to meet you where you’re at, and guide you through an effective and tailored treatment plan that has incredible success rates.
Relationship OCD (ROCD) is an OCD subtype in which the sufferer is plagued by distressing and persistent doubts about their most valued relationships. These unwanted obsessions thrive in the uncertainty surrounding the quality of the relationship and their love for their partner or child.
Postpartum/Perinatal OCD is the subtype used to describe those who struggle with OCD following childbirth or during their pregnancy.
The sufferer may or may not have experienced OCD prior to their pregnancy however, what characterizes postpartum and perinatal OCD is the obsessional fears surrounding their newborn child.
Those obsessions can affect anyone, regardless of gender or whether or not they actually birthed the child.
While it is predominantly mothers who experience this particular strain of OCD, it can affect fathers and cares providers in the same way.
The level of shame that accompanies this particular subtype is incredibly painful as intrusive thoughts can take the form of harmful intrusive thoughts and sexual intrusive thoughts.
Because of this, many avoid seeking help for fear of judgment and fear of being reported for their thoughts. While they know they feel disgusted and tormented by these thoughts, they worry that someone may misconstrue them for liking those obsessions.
When you work with a trained OCD specialist, you are welcomed and supported without judgment.
Our clients come to us with these same fears but we quickly show them that they are in a safe, non-judgmental space. Please get in touch with our highly trained team of mental health professionals if this resonates with you, and we will conduct a thorough diagnosis and ensure you receive the highest standard of treatment.
Postpartum OCD is also now commonly referred to as Perinatal OCD, as obsessions can begin during pregnancy. For the purpose of this article, any mention of postpartum OCD also refers to perinatal OCD and may be abbreviated to PPOCD.
What is Postpartum OCD?
Postpartum OCD typically develops rapidly as the sufferer realizes they are suddenly responsible for a new life, or about to be.
As with any OCD, sufferers are tormented by unwanted obsessions which they attempt to alleviate by engaging in compulsive behaviors.
For those with postpartum OCD, their fears are directly related to that of their newborn child. Having an immense new sense of responsibility for a person can feel like a lot of pressure.
Added to this, your newborn is a source of love and joy. The unconditional love we have for our children is unparalleled by anything else. It is because of this love that OCD can thrive in new mothers or fathers.
Being egodystonic in nature, OCD goes against the sufferer’s values which is why those intrusive thoughts feel so alarming and disturbing. Obsessions play on our fears about the thing we love most or hold in high value, in this instance, our new child.
In OCD, we are always tormented by uncertainty.
It is the uncertainty surrounding those obsessions that cause us to fixate and try to solve them, which keeps the cycle in motion.
But when you have strong urges or fears of harming your child in some way or experience a groinal response while breastfeeding or changing your child’s diaper, it’s not surprising that you would want to find some sort of definitive guarantee that you can keep your child safe.
However, those physical or mental compulsions done to gain that sense of certainty keep the OCD cycle in motion.
It is in learning how to change your relationship to those obsessions and resisting the urge to do compulsions that you can finally find joy in raising your child.
Studies have shown that biological factors (such as genetics) and environmental factors (such as upbringing and stressful life events) often combine to trigger the onset of OCD.
The important thing to understand here is that we do not need to deep dive into the reason why you have this condition. When clients come to us, our team of compassionate OCD specialists uses the top methodologies that are proven to yield incredible results in OCD recovery.
Postpartum OCD Symptoms
Postpartum Obsessions
Postpartum OCD thoughts involve urgent, intrusive thoughts surrounding the possibility of something bad happening to your baby, either at the hands of yourself or someone/something else. These intrusive thoughts feel devastating and take up much of your time and focus.
Feeling triggered by stories of mothers who have harmed their babies, wondering, “what if that’s me?”
Those with postpartum OCD experience Harm OCD urges, which involve sensations within the body that make you feel as if you may want to or will harm your baby. For people with OCD, urges may convince them that they are “capable” of harming someone, despite being terrified at the idea of doing so.
Some mothers experience a groinal response when breastfeeding and fear that it means that they are sexually attracted to their child in some way even though they find the thought abhorrent.
OCD thoughts, feelings, sensations, images, and urges may also involve dissociation, derealization, or depersonalization.
High levels of shame and guilt, loss of identity, and low self-esteem due to the constant questioning of your character.
Fears of dropping the baby, harming the baby, leaving the baby in a strange place, the baby getting sick, the baby dying in their sleep, etc.
Googling “what if I think about harming my baby?” etc.
Asking your loved ones if you’re a bad mother or a violent person
Reassuring yourself by saying things like, “I would never harm my baby”
Self-punishment: Criticising yourself for your thoughts and how you feel as a new parent.
Excessive and repetitive reassurance-seeking from friends and family that you are not a bad parent and are doing a good job.
Checking on your baby constantly throughout the night to make sure they’re okay
Refusing to let anyone else care for the baby
Mentally ruminating on whether you are capable of harming your baby
Struggling to sleep and battling with restless nights due to relentless intrusive thoughts
Being hyper-aware of every move you make, and mentally checking for the intentions behind your behaviors.
Avoiding objects, places, or activities that could encourage you to commit harm, such as:
Crowded places
Knives
Giving your baby a bath
Avoiding your baby as much as possible for fear of what might happen if you lose control
Click here to join our newsletter and receive instant access to our 6-part mental compulsions audio series where you will learn how to resist the urge to perform mental compulsions (with PDF worksheets)
What does Postpartum OCD feel like?
Those with PPOCD commonly experience feelings of overwhelm, shame, guilt, exhaustion, and isolation.
The clients who come to us with this subtype are good mothers (and fathers). More to the point, they want to be great parents. For many, especially for their first child, it is a life milestone they’ve been craving only for it to arrive and OCD feels like it has stolen happy memories from them.
All these clients want for themselves is to be with their new child without drowning in fears. Fears that stop them from living in the present moment and creating happy memories with the one they love most, their newborn.
Many face this battle alone which feels incredibly isolating.
Especially for those with harm obsessions or sexual obsessions, the feeling of shame that arises is gut-wrenching.
As with other subtypes that experience such obsessions, like pedophilia OCD or sexual orientation OCD, the sufferer often feels scared to share their struggles for fear of being misunderstood.
It’s important to know that OCD attacks your values and goes against your nature.
This is why those intrusive postpartum obsessions are so terrifying, it’s because you don’t want them to become a reality.
Thoughts are not facts. Just because you think them does not make them true.
Anxiety and uncertainty are not a sign that you are in danger
You are more than your obsessions and compulsions
You are stronger than your OCD
You can break the cycle of OCD by creating a clear plan of attack and standing up to OCD
What’s the difference between normal mother fear and Postpartum OCD?
Every new mother (or parent) experiences worries about the safety of their newborn, this is perfectly natural.
It’s an innate response in us as humans to want to protect those we love and when it comes to a new child, there’s no one who needs greater protection.
However, for those with postpartum OCD, the fear and uncertainty of what might happen can leave them hopeless and helpless. They do not feel confident in leaving those doubts unexplored because the fear of potential consequences if they were to become a reality, is too strong.
Postpartum OCD can haunt every moment with a newborn.
It feels relentless and overwhelming, constantly tormenting the sufferer, and this stops them from enjoying the experience of parenthood.
What some might consider typical mother fear may come in ebbs and flows and those fears can be brushed aside as they engage in connection and bonding. Those fears can feel never-ending and all-consuming.
How is postpartum OCD diagnosed?
There is no test for postpartum OCD, but there are tests for OCD.
This is because all OCD, PPOCD related or otherwise, are treated the same.
No matter the content of your OCD, we’re looking to identify obsessions and compulsions as well as their severity using the Yale-Brown Obsessive Compulsive Scale (Y-BOCS). We can then identify the area in which your obsessions are focused on.
During the assessment phase, our trained clinicians (or other OCD specialists) will perform a formal assessment of OCD and other coexisting disorders and make sure you are given a correct diagnosis so that you can receive the best possible treatment.
How is Postpartum OCD treated?
When a patient or client comes to therapy, the first question they often ask is, “Will Postpartum OCD go away?” or “Please, tell me how to stop prenatal OCD thoughts?” or “Tell me how to make these urges to go away?”
While these requests are entirely understandable given how scary those obsessions are, our clinicians begin by providing psychoeducation and self-compassion training to our clients so they can learn that this is not the goal in OCD recovery.
Given the high levels of guilt and shame related to PPOCD we highly emphasize the importance of self-compassion training to help manage the strong emotions our client’s experience.
Instead, using the below treatment tools, people with OCD learn how to change their relationships and response to their obsessions (which is within our control), instead of trying to stop them completely (something that is not in our control).
The ultimate goal of postpartum OCD and perinatal OCD recovery is to help you feel comfortable and confident in being with your new son or daughter so you can capture those joyous moments throughout their early years.
We place focus on building a value-based life and not living according to what our OCD fears tell us to do.
This means being able to breastfeed without fearing the groinal response.
This means meeting up with friends at a cafe and doing the things you would choose to do if OCD were not present.
This means picking them up and holding them close and creating beautiful memories.
It means enjoying the time you get to spend bonding with your child without fear and panic stealing your attention and precious moments.
Best treatment for Postpartum OCD
Overcoming OCD can feel impossible, but rest assured, it’s far from it. The gold-standard approach to OCD treatment and OCD recovery is Exposure and Response Prevention therapy (ERP) which is a type of Cognitive Behavioral Therapy (CBT).
The cognitive portion of CBT refers to the identification of distorted thoughts and learning to restructure them into more reasonable, rational thoughts. The behavioral portion is where ERP comes in. OCD treatment requires that we focus mostly on the behavioral component, as this has the best clinical outcomes.
The practice of ERP involves the creation of a hierarchy.
This hierarchy is developed together by the therapist and client. Once the client has been educated on how to manage their thoughts, feelings, sensations, and urges, they will then begin re-engaging with a daily routine that aligns with how they wish to spend time with their child.
The purpose is to practice tolerating thoughts and resisting the urge to engage in compulsions.
Common examples of ERP for postpartum OCD might look like:
Talking and singing to your child while changing their diaper without ruminating on whether you will cause your baby harm
Going to the park and resisting the urge to ruminate on thoughts like ‘what if I accidentally leave them here’ or ‘what if they get sick from germs in the sand pit’
Focusing on getting better sleep and decreasing the number of times you check on your baby throughout the night
During treatment, our clinicians will teach you to use skills such as mindfulness, Acceptance and Commitment Therapy (ACT), and Self-Compassion.
Recent studies have shown that incorporating mindfulness into CBT and ERP improves recovery outcomes.
Mindfulness involves experiencing your thoughts, emotions, and physical sensations, from a non-judgmental, “right now” perspective. Mindfulness is a tool that can be used anywhere, in any situation.
It might feel scary to begin this treatment however, it only takes a moment of courage to get the ball rolling.
With every compulsion you engage it, you strengthen OCD’s hold. For Postpartum OCD, time can be against you. You want to enjoy being with your new child and you want to crystallize beautiful memories that you can look back on in fondness.
So while you may not feel ready, the time to take action is now.
You can see incredibly fast results with the correct treatment, which means you can alleviate those feelings of shame, feel like the good parent we know you are, and experience parenthood the way you want to sooner than you think.
If you want support with this, here is how we can help you…
1:1 Therapy for Postpartum OCD
Our team of highly skilled OCD clinicians are here to support you in your postpartum OCD recovery, without judgment.
We can work with any sufferers in the areas of California to create a specialized treatment plan that utilizes the best methodologies for proven results.
Under the supervision of top OCD specialist Kimberley Quinlan, we can help you feel confident and comfortable to experience those precious moments with your newborn without fear.
Online self-study course for OCD recovery
If private therapy is currently unavailable to you, Kimberley Quinlan has created ERP SCHOOL.
An affordable and accessible self-study program that will give you the exact tools Kimberley uses with her private clients to help them overcome OCD.
It combines the best methodologies that are proven to yield incredible results in OCD recovery. You will understand how to apply these tools and techniques to your postpartum OCD and begin to resist the urge to do compulsions.
We do not want you to feel like you need to avoid your child, feel immense shame around your intrusive thoughts, or limit your experiences with your newborn…
You can stop letting intrusive thoughts ruin your experiences of parenthood and resist the urge to do compulsions so you can have a happy life with the ones you love most.
Existential OCD is characterized by excessive fear, worry, and uncertainty surrounding life and death. People with this OCD subtype find themselves trapped in thoughts about the meaning of life, the purpose of one’s existence, what’s real and what isn’t, and what happens when they die.
Philosophy, as a study, intentionally poses and ponders these questions. This is why existential OCD is sometimes known as philosophical OCD.
Pedophilia OCD (POCD) refers to a common OCD theme in which one fears being sexually attracted to and/or sexually harming children.
It is distinctly different than pedophilia disorder.
OCD is egodystonic in nature.
This means that its obsessions inherently go against the sufferer’s true values or desires. In the context of pOCD, alarming, sexual, intrusive thoughts arise that are disturbing in nature, leaving the sufferer questioning why they would think these thoughts and whether they could do such acts.